
Case Report | DOI: https://doi.org/10.31579/2690-8794/042
*Corresponding Author: Monteiro Zappelini C. E., PhD in Otorhinolaryngology, Otorhinolaryngologist and Professor of the Medicine Course at University of the Southern Santa Catarina (UNISUL), Brazil.
Citation: de Carvalho G. C., Niero C., Monike R. Medeiros, da Silva V. E., Freitas Marcelino T. D. and Monteiro Zappelini C. E., Maxillary mucocele – unusual localization J, Clinical Medical Reviews and Reports. 2(7); DOI: 10.31579/2690-8794/042
Copyright: ©2020, Monteiro Zappelini C. E., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 July 2020 | Accepted: 31 July 2020 | Published: 30 September 2020
Keywords: mucocele; maxillary sinus; para nasal sinuses
Mucoceles of the paranasal sinuses are benign expansive cystic lesions, originated from the obstruction of the nasal drainage, have mucous or mucopurulent secretions and are covered by respiratory epithelium. Its development is insidious, generally unilateral and has a higher incidence between the third and fourth decades of life, with no gender predilection.
Objective: To present a rare case of mucocele in the maxillary sinus, addressing the methods used in diagnosis and treatment.
Final comments: The clinical evaluation associated with imaging tests suggest the diagnosis of mucoceles and the definitive treatment must be surgical.
Mucoceles of the paranasal sinuses are expansive and benign cystic lesions, which occur due to obstruction of the nasal drainage, with varied etiology, whether due to chronic sinusitis, polyps, bone tumors, post-traumatic, neoplastic obstruction, post-inflammatory complications or after surgical intervation [1, 2]. These lesions are lined by respiratory epithelium and have mucous or mucopurulent secretions inside [3, 4].
The development of the mucocele is insidious, in most of the cases unilateral, presenting a higher incidence between the third and fourth decades of life, with no gender predilection [5, 6]. It can occur in any paranasal sinus, being more common in the frontal and ethmoid, followed by the sphenoid sinus. It has a rare incidence for its development in the maxillary sinus (between 3 and 10%), with the history of previous surgeries at the site being the factor most associated with its appearance [7, 8].
All mucoceles have two stages of development, which are represented, first, by clinical latency, followed by externalization or complication, a stage which they expand outside the limits of the affected sinus. [7, 9] And, despite presenting a benign course, they can be very harmful, leading to local bone resorption due to increased pressure on the bone [10].
The clinical presentation of the maxillary sinus mucocele may present in the form of cheek bulging, diplopia and dental problems, even if they generally do not present pain, except in cases of infected mucocele [11]. In the clinical latency phase, its diagnosis is accidental, when perform a computed tomography (CT) scan of the paranasal sinuses [12]. Mucocele treatment should always be surgical, with the access route chosen depending on its location and the involvement of neighboring structures [7, 9].
The objective of this work is to present a rare case of maxillary mucocele, addressing the methods used in diagnosis and treatment.
A white, 41-year-old male patient arrives at the otorhinolaryngology outpatient clinic reporting a history of pain and swelling in the right maxillary region with an evolution of the condition in 2 months. Patient denies any comorbidities or previous surgeries. On physical examination, he presented an increase in volume in the right maxillary region, which was slightly painful on palpation. The exams of anterior rhinoscopy, oroscopy and video- nasofibroscopy performed in the office did not show any changes. As complementary exams, computed tomography (CT) and magnetic resonance imaging (MRI) of the sinuses were requested.
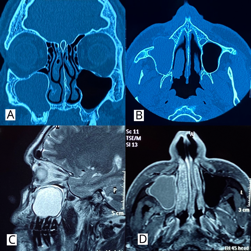
CT analysis shows an oval image of thin walls and calcified walls, with an insufflating aspect. The content inside it is a thick and homogeneous liquid that affects the right maxillary sinus, extending through the anterior wall of the maxillary sinus to the subcutaneous tissue of this region. The lesion measures approximately 4.1 x 4.0 x 2.6 cm.
The other paranasal cavities present normal aeration. It is also possible to highlight a minimal deviation of the nasal septum to the left, with the formation of a large ipsilateral bone mass, touching the inferior nasal turbinate on this side and obliterating the respective nasal meatus. The middle nasal turbinate are bilaterally paradoxical.
Through the analysis of MRI of the paranasal sinuses, the filling of the right maxillary sinus is observed with material that presents low signal at T1 and high signal at T2, inferring high water content, promoting bone remodeling of its walls, with anterior extension of the content due to discontinuity of the anterior wall from the maxillary sinus to adjacent soft tissues. There is peripheral enhancement to the paramagnetic contrast agent. The diagnosis impression was mild mucosal thickening on the floor of the left maxillary sinus and slight deviation of the nasal septum to the left, with ipsilateral bone mass.
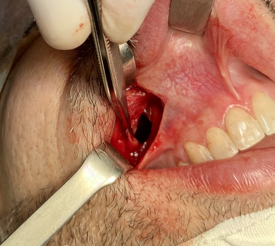
From the clinical and complementary examination, it was possible to establish the diagnosis of maxillary sinus mucocele. Surgery was performed with an external approach (Calwell-Luc) and endonasal endoscopy (right maxillary antrostomy)
The anatomopathological examination showed a non-specific chronic inflammatory process, with fibrous proliferation, edema in the maxillary sinus and absence of cells with malignancy.
The patient is being followed up, with no recurrence after 6 months of surgery.
Despite being benign and rare, mucocele of the maxillary sinus must be approached surgically due to the potential of being locally aggressive, evolving with bone destruction in the orbital and also dental regions [5]. It has several predisposing factors such as chronic sinusitis, previous surgery, allergic rhinitis and nasal trauma. However, some patients have no identifiable cause. The disease can present with a variety of symptoms that are generally related to its expansion and subsequent pressure on the surrounding structures [10].
To make the diagnosis, Computed Tomography was the eligible exam and is also the gold standard, being fundamental, since the patient's clinic can be scarce and nonspecific [2].
In the report presented above, the local increase and pain on palpation were the first signs and symptoms reported by the patient, which agrees with the literature. A series of thirteen cases of mucocele of the maxillary sinus concluded that this clinic was present in 77% and 69% of those affected, respectively [14]. In addition to these manifestations, other case reports also highlighted the presence of mucopurulent fluid drainage into the nasal cavity, nasal obstruction, rhinorrhea, headache, amaurosis and diplopia. [14, 15, 16, 17].
What attracts attention in the case presented is the absence of a history of trauma and previoussurgery.
The epidemiology of this disease indicates prevalence between the third and fourth decades, according to the case reported. Among the reports analyzed, the age group in which most cases are found was between the third and seventh decades [14, 15, and 16].
The endonasal endoscopic approach associated or not with Caldwell-Luc external access is an effective and safe method for the treatment of the lesion, and most patients have symptom resolution without need of a new surgical intervention [10].
Despite being a rare condition, the maxillary sinus mucocele must be among the diagnostic hypotheses considered in clinical reasoning when faced with an increase in the malar region and pain on palpation at that location. Often, diagnosis and treatment is carried out with a multidisciplinary team of doctors, especially the otolaryngologist, and the buccomaxillofacial dentist. Computed tomography is the exam of choice, and the therapeutic approach is always surgical, with marsupialization of the mucocele lining, in order to avoid recurrences.
Finally, the purpose of constructing this report was to expose to the scientific community a case of unusual location of the mucocele otorhinolaryngological practice, with little progress.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
